
Access to Justice and Public Attorneys’ Role in Right to Health Litigation in the City of São Paulo
Right to health litigation in Brazil raises a debate regarding its distributive effects in a resource-constrained setting. Several studies have found that a significant proportion of litigation features individual claimants who live in the most affluent states, cities and districts of Brazil and are usually represented by private lawyers, whose fees are beyond the reach of most of the poor population. For some, this is an indication that the distributive effects of litigation are very likely negative because litigation tends to benefit a privileged socio-economic group and may force health authorities to divert to them resources from comprehensive health programs that benefit the majority of the population. Others, however, argue that courts can nonetheless provide an important institutional voice for the poor and promote health equity when they manage to access them. The main problem for this “pro-litigation camp” is thus to enhance access to Justice. Our aim is to analyze lawsuits in which litigants are represented by public attorneys in right to health litigation in the city of São Paulo to inquire if at least this type of litigation is reaching out to the neediest citizens. This study analyzes three indicators: the income of litigants, the Human Development Index and the Health Need Index of the areas where they live. Our conclusion is that although public attorneys seem to represent mostly low income people, other indicators suggest that there are still important obstacles for public attorneys to reach the neediest.
Since the recognition of the right to health in the 1988 Brazilian constitution, and more intensely from the 2000s onwards, hundreds of thousands of lawsuits have reached the Brazilian courts asking the judiciary to enforce that right against government.1 There is a growing interest in academia in studying the characteristics of this phenomenon and also its impact in the actual enjoyment of the right to health by the Brazilian population.
The more general picture in Brazil so far (FERRAZ, 2011a, 2011b) has shown that litigation is overwhelmingly concentrated in states, municipalities and districts where socio-economic indicators, and health conditions as a consequence, are comparatively better. There is also evidence from some studies that the bulk of expenditure incurred by government through litigation concentrates on individual treatments, often imported and mostly expensive drugs for conditions that are arguably not a priority for the majority of the population served by the public health system (VIEIRA; ZUCCHI, 2007; CHIEFFI; BARATA, 2009; MAESTADT; RAKNER; FERRAZ, 2011; NORHEIM; GLOPPEN, 2011). Furthermore, there is strong empirical evidence that in most localities litigants claiming health treatments come mostly from privileged backgrounds (VIEIRA; ZUCCHI, 2007; SILVA; TERRAZAS, 2011, CHIEFFI; BARATA, 2009; MACHADO et al., 2010; MACEDO; LOPES; BARBERATO-FILHO, 2011; PEREIRA et al, 2010; SANTOS, 2006).
According to these studies, therefore, the judicialization of health in Brazil tends to benefit a privileged socio-economic minority who have easier access to information, to legal assistance and to courts, likely forcing health policy authorities to divert scarce resources from comprehensive and rationally devised health programs that benefit the majority of the population to health services (often new and expensive drugs) that are neither cost-effective nor a priority for a public health system that aims to serve a large and needy population with limited resources (VIEIRA; ZUCCHI, 2007; CHIEFFI; BARATA, 2009; FERRAZ, 2009, 2011a, 2011b; MAESTADT; RAKNER; FERRAZ, 2011; NORHEIM; GLOPPEN, 2011).
This “Brazilian model” of health litigation (FERRAZ, 2009, 2011a) has divided commentators into two opposite camps. On one side, there is the pro-litigation camp, which believes that litigation plays a legitimate and positive role in forcing a recalcitrant executive to comply with the right to health included in the 1988 constitution. Others, however, claim that the kind of litigation that is prevalent in Brazil (the “Brazilian model”), rather than make the right to health effective, might represent a hindrance in the implementation of that right.2
We want to assess more thoroughly in this article one of the claims of what we call the “pro-litigation camp” which seems to us, at least in principle, plausible. Before that, however, we must first distinguish between two main strands within the pro-litigation camp that are significantly different (our article engages only with one of these strands). One position (defended mostly by lawyers, judges and some health rights activists) simply overlooks or ignores as irrelevant the picture emerging from the empirical studies above cited. For them, the “Brazilian model” of litigation is not at all problematic in that, even if benefiting mostly a comparatively privileged socio-economic minority, it is still, in their view, enforcing the right to health recognized in the constitution, which doesn’t distinguish between poor or rich, i.e. is a universal right. We find that position untenable for reasons that we can only briefly indicate here. Given that resources for health are necessarily scarce (i.e. resources available in the Brazilian public health system are not sufficient to satisfy all health needs of the whole population), the right to health recognized in the Brazilian constitution cannot be plausibly interpreted as an unlimited right to the satisfaction of every health need of the whole of the Brazilian population (FERRAZ; VIEIRA, 2009). Moreover, in highly unequal countries like Brazil, where there are huge historical inequalities in health and all other social goods which the constitutions aims to reduce (article 3), the right to health cannot be interpreted in a way that is neutral to the needs of the poorest. Such “neutral” interpretation would either perpetuate these huge health inequalities or, worse, increase them, as the Brazilian model of litigation is probably doing, although perhaps not, or not yet, on a massive scale (FERRAZ, 2009).
The other main position within the pro-litigation camp is much more plausible. It accepts all the premises of the anti-litigation camp, i.e. that resources are scarce, that they need to be allocated in a non-neutral way so as to improve the health conditions of the poorest, and that the Brazilian model of litigation is not ideal. Yet they believe that the model is not entirely negative, and have an optimistic view about the possibility of changing it for the better.
One of their arguments is that courts can (potentially at least) provide an important institutional voice for the poor provided that access to them is extended to the least advantaged. The solution, thus, should not be to stop litigation, as some critics of the judicialization of health seem to suggest, but rather to extend it to those who need it most. In other words, the problem is not with litigation itself, but rather with access to Justice. Thus, if significant improvement in access to Justice occurred, litigation could in principle have a positive impact.
This is the hypothesis we test in this article. Access to Justice has indeed improved to some extent in Brazil since the 1988 constitution. Regarding right to health litigation, there are two states where litigants represented by public attorneys surpass those with private representation: Rio de Janeiro and Rio Grande do Sul (PEPE et al., 2010; SANT’ANNA, 2009; MESSEDER; OSORIO-DE-CASTRO; LUIZA, 2005; BIEHL et al., 2012).3 In the case of the city of São Paulo, between 25-30% (SILVA; TERRAZAS, 2011; CHIEFFI; BARATA, 2009) of the claimants are represented by public attorneys of the Public Defender’s Office (Defensoria Publica, hereafter “DP”) and Public Prosecutors’ Office (Ministerio Publico, hereafter “MP”), whose remit is exclusively (DP) or in part (MP) to represent the most disadvantaged.
We use empirical data collected in 2009 at the DP and MP in the city of São Paulo on the socio-economic profile of litigants and the types of health benefits claimed through litigation. Our aim is to determine whether these public attorneys are capable of effecting the changes that the more plausible position within the pro-litigation camp claims to be feasible. If there are any actors who are capable of using litigation to improve healthcare policies for the needy, they will probably be these public attorneys.4 Assuming as correct our non-neutral interpretation of the right to health, our questions are these: i. have public attorneys so far represented those who to be most in need? ii. have they focused on the health issues that are most urgent in order to improve the health of the poorest groups of the population?
The city of São Paulo was chosen as the case study in this paper for several reasons. Firstly, due to the availability and accessibility of data. Secondly, because São Paulo is one of the cities where health litigation is most rampant, partly because it is the biggest city in Brazil in terms of population and wealth, and has also a reasonably well developed public health system. Lastly, most empirical research showing a strong relationship between socio-economic status and volume of litigation was carried out in São Paulo. Hence, it is possible to use São Paulo to compare health litigation initiated by private lawyers on behalf of comparatively advantaged individuals with that initiated by public attorneys in order to gauge if the claims of the pro-litigation camp stand or not.
The DP is the institution responsible for providing free legal assistance to low income citizens who have no economic resources to pay for private lawyers. In the state of São Paulo, specifically, this institution was created only in 20065 and offers legal assistance to citizens whose monthly household income is not more than three times the national minimum wage.
When the data collection was concluded, in the end of February of 2009, the national minimum monthly wage was R$ 465 (Brazilian reais), so the threshold for qualifying for free legal assistance from the DP was R$1,395,00 per month the equivalent of around US$580 then. However, this threshold is flexible and people above this it can still qualify for legal assistance depending on their family situation (assets and number of members), the economic value involved in litigation and the type of litigation. Particularly in cases involving medication, the threshold can be (and often is) set aside when the price of the medication litigated is high.
The DP has many units spread around São Paulo City, but right to health cases are centralized in one unit (Unidade Fazenda Pública) at the heart of the city center. In this unit there were in 2009 five Public Defenders and cases were randomly distributed to each of them, which means that they were responsible for approximately the same number of cases. Given this distribution, analyzing the cases for which one particular Public Defender was responsible provided us with a random sample of 20% of all right to health cases in the DP.
We selected right to health cases from 2006, the year when the Public Defender’s Office went into operation in São Paulo, until February of 2009, when the research was concluded. In total, 340 cases were analyzed.
The MP is the institution responsible for, among other tasks, ensuring respect by public authorities for the rights guaranteed in the constitution and for protecting and representing collective and public interests.6 Although both the DP and the MP have standing to bring individual and collective lawsuits, an informal agreement between them established that, in São Paulo, the DP would be mainly responsible for individual lawsuits, whereas the MP would be mostly focused on class actions (Ações Civis Públicas).7
In the MP, at that time, there was a special department responsible for right to health cases: the Group for Special Action in Public Health (Grupo de Ação Especial à Saúde Pública, acronym GAESP).
GAESP was created in 1999 and until the date when the research was concluded, February of 2009, it had lodged 62 class actions. Among these actions, we chose only those in which litigation was against public authorities and demanded some sort of public provision of health care or other health related measures (32 cases fit this description and were thus analysed).
In the cases represented by the Public Defender’s Office, most cases (47%) involved a claim for drugs for the following health problems: Diabetes (25,24%), Cerebral Palsy (6,65%), Arterial Hypertension (5,48%), Glaucoma (3,32%), Cerebrovascular Accidents (3,33%), Heart Diseases (3,33%), Cancer (2,35%). There was also a significant volume of cases demanding health products for Diabetes measurement and control, and diapers for people who suffered from Cerebrovascular Accidents and Cerebral Palsy.
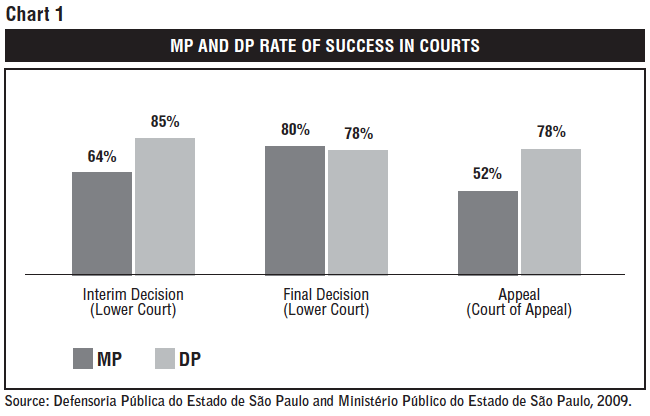
In most cases the DP had a successful result. Among the 293 cases in which this information was available, in 84.64% of them the Public Defender got an interim decision in favour of the claimant. In 78% of the cases the final judgment was in favour of the claimant. The data also show that there were 187 appeals lodged by the government of the State of São Paulo in the Court of Appeal against unfavorable final judgments. The result of the appeals was available in 63 cases and were unsuccessful (i.e. against the State) in 76% of them. According to the DP’s records, in only 27 cases the first instance decision went against the claimant, but after these cases were appealed, the result was reversed in favor of the claimant in 21 cases, i.e. almost 80%. Thus, according to the data available, patients’ total rate of success in the Court of Appeal was around 78%.
The Public Prosecutor’s Office Group for Actions in Public Health (GAESP) lodged exclusively class actions (Ações Civis Públicas). Among the 32 cases analyzed, 22 (69%) were complaints about the bad conditions of public health hospitals, basic health units and clinics. The causes of the litigation are lack of materials, instruments, medicines,8 ambulances, equipment, professionals (doctors and nurses) and problems with the buildings’ hygiene, safety and maintenance.
In 9 cases (28%) the Public Prosecutors’ Office demanded specific medicines and treatment for the following diseases: Hepatitis C (2 lawsuits), Malignant Hyperthermia, Chronic Renal Failure, Epilepsy, Chronic Obstructive Lung Disease, Autism and Adrenoleukodystrophy. In one case it demanded free public transportation to medical facilities for low income pregnant women.
The information about the cases’ rate of success was not available for the whole dataset. For the first instance, this information was available in 66% for interim decisions, 76% for final decisions and 63% for appeals. The result was that, according to the data available, 64% of the interim decisions were decided in favour of the claimant and 36% against. Concerning final decisions, 80% were decided in favour of the claimant and 20% against. Regarding appeal decisions, the rate of success for claimants falls to 52%.
The comparison between the rate of success shows therefore that the MP is significantly less successful than the DP both in interim decisions in the lower courts and on appeal of final decisions in the Court of Appeal, yet slightly more successful in final first instance decisions (See Chart 1).
The higher reversal on appeal and the lesser success in interim decisions for MP cases could be explained by the fact that these cases are collective and therefore more structural than those lodged by the DP. They are structural in the sense that they aim to promote significant changes in the public health policies that will affect a larger number of people and will have significant economic and budgetary impact, whereas the DP cases in our sample are all individual claims.
As a general rule, it is possible to affirm that the higher the political and economic impact the more cautious courts (especially high courts) will be in reviewing administrative and political decisions (see TAYLOR, 2006, p. 275). This could be explained by the fact that in these cases courts are less certain about the consequences of the decision or because judicial activism in these cases could bring them into serious conflict with political branches. That is probably the reason why small scale demands – for example, the individual claims lodged by the DP – are more prone to success than structural cases, as are also the individual cases lodged by private lawyers. It is true, of course, that individual cases can in the aggregate have significant impact on policy and budgets as well, especially when there are thousands of them, but this potential indirect effect does not seem to concern judges.
The Brazilian Federal Supreme Court (the highest court in the Brazilian judicial branch) seems to confirm this general rule, at least in right to health litigation. In two recent decisions – STA 424 and SL256 – the Federal Supreme Court rejected collective complaints on the grounds that they may affect the public budget and be an “obstacle to the adequate provision of public services by the Public Administration”. This court also affirmed that a healthcare claim should be granted only if the need is proved individually. Even though the Federal Supreme Court interpretation does not bind lower Courts (save few exceptions), these decisions can be used as an example of a certain behaviour in Courts that may explain why lawsuits lodged by the MP are, in general, less successful than those lodged by the DP.
Poverty is not an easy phenomenon to assess. Different interpretations of reality translate into different poverty measures. Hence the question whether a certain group is poor and how poor it is will allow many answers depending on the understanding of poverty and the “space of concern” that is being measured (LADERCHI; SAITH; STEWART, 2003, p. 244). The data available in the files at the DP offer us two indicators that can be used to assess the socioeconomic status of those represented by this institution: household income and the district where litigants live.
Because the DP services are in principle restricted to those below a certain household income threshold, all citizens who wish to receive free legal assistance have to declare and, at least in principle, bring evidence of their household income (as opposed to individual (per capita) income).9
Since the number of family members was not widely available, we decided to use the average number of family members in the metropolitan area of São Paulo – 3.2 persons per family (DIEESE, 2009) – as the best (though not perfect) proxy to define our sample’s income per capita. This was important because income per capita is one of the most widely used indicators of poverty allowing us to compare the socioeconomic status of our sample with the population as a whole.
We are aware that even though the monetary approach is the most frequently used, it has some important limitations. There are other aspects of human deprivation that do not depend exclusively on the amount of money someone owns (SEN, 1992). For example, citizens with a lower income may have better health outcomes than those with higher incomes if the former have access to good public health services whereas the latter have to pay for it or have to travel long distances to receive health care.
For this reason, we will also use the Human Development Index (HDI) and the Health Need Index (HNI)10 of the districts where the claimants in our sample live to shed some light on aspects that the purely income based analysis cannot show.11
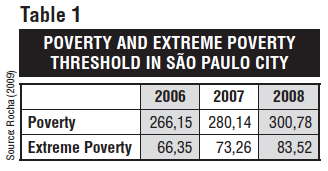 The poverty and extreme poverty threshold we use in this paper were developed by Rocha (2009) for the urban area of the city of São Paulo. She defines the extreme poverty threshold as the amount of money needed by a person to purchase a minimum quantity of food. The poverty threshold is in turn calculated as the amount of money a person needs to fulfill her basic needs, such as food, transport, leisure, health, education and hygiene.
The poverty and extreme poverty threshold we use in this paper were developed by Rocha (2009) for the urban area of the city of São Paulo. She defines the extreme poverty threshold as the amount of money needed by a person to purchase a minimum quantity of food. The poverty threshold is in turn calculated as the amount of money a person needs to fulfill her basic needs, such as food, transport, leisure, health, education and hygiene.
The thresholds’ values in Brazilian Reais for the city of São Paulo are described in table 1.
Chart 2 shows the distribution of litigants’ socio-economic status according to the year of the lawsuit. As stated above, the individual income was calculated by dividing the declared household income by the average number of persons per family in the metropolitan area of São Paulo, which is 3.2:
This chart shows that most of those represented by the DP are below the poverty threshold line if we assume that their self-declared income is accurate (see however the comment below). Considering the proportion of people below this threshold (including the extremely poor and the poor) in São Paulo City’s whole population – 2006 (22%); 2007 (20%); 2008 (19%) – (ROCHA, 2009), it could be affirmed that the DP services are reaching significantly the lowest income quintile of the metropolitan area of São Paulo. Around 80% of those represented by the DP belong to the 20% poorest people in the city of São Paulo.
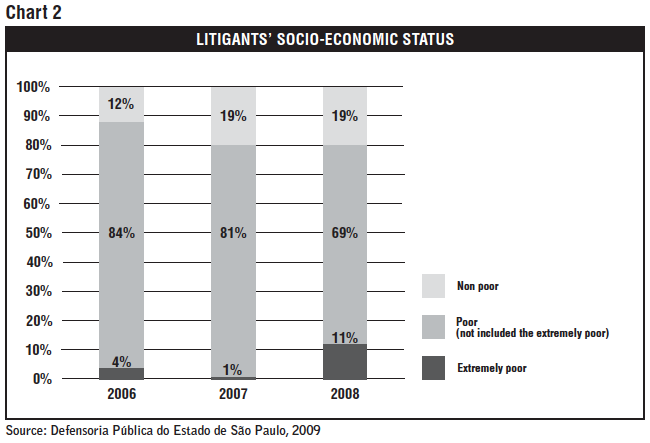
It is also true, however, that only a small number of cases feature individuals below the extreme poverty threshold. Although their proportion in the population is also low – 2006 (3%); 2007 (3%) and 2008 (2,9%) (ROCHA, 2009).
As already mentioned, however, income alone is not necessarily an accurate indicator of deprivation. Moreover, even though applicants for free legal assistance need in principle to take documents to prove their low income (e.g. employment contract or social insurance benefit slips) the data on income available from the lawsuits are mostly based on self-declaration and, as we will see, might thus not reflect the real income of those represented by the DP. In the following sections we use two other indicators to test the results reached through income alone.12
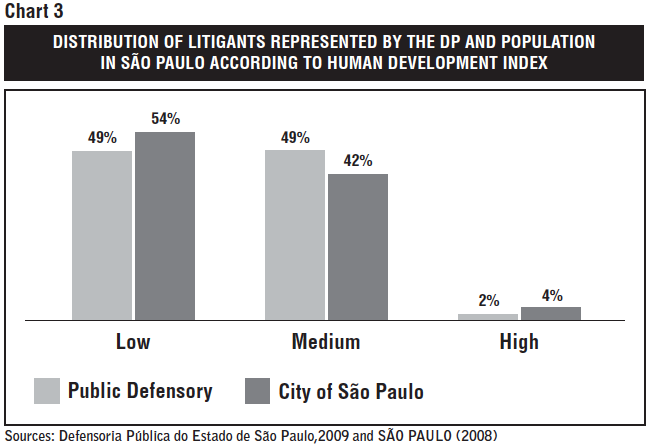
The human development index aims to measure a population’s quality of life in a comprehensive way, including GDP per capita, life expectancy and educational attainment.
In the city of São Paulo, 4% of the population lives in districts with high HDI (above 0.8), 42% in districts with medium HDI (between 0.5 and 0.8) and 54% in districts with low HDI (below 0.5). In our litigants represented by the DP, people who live in areas with low HDI are slightly underrepresented whereas those who live in districts where the HDI is medium are considerably better represented (See Chart 3).
The Health Need Index (Indice de Necessidade em Saúde) was developed in order to identify which areas of the city of São Paulo should be prioritized in the distribution of health care services. It is calculated using data related to demographic, epidemiologic and social conditions in each district. The districts are distributed according to the level of their health needs. The higher the HNI, the more urgent are the population health needs (SÃO PAULO, 2008).
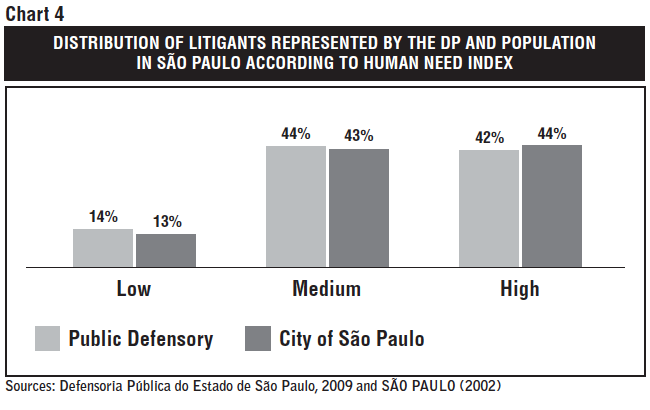
In our sample, only 42% of litigants represented by the DP live in areas in which health needs are high, and thus where implementation of the right to health is arguably more deficient (Chart 4). The majority of cases (58%) feature litigants who live in areas regarded as of medium or low HNI.
The data presented above brings up interesting but at points contradictory aspects of right to health litigation sponsored by the DP. If we take into account the self-declared income of litigants, it would seem that the vast majority of lawsuits brought by the DP (more than 80%) feature individuals who are below the poverty threshold of the city of São Paulo and belong to the lowest quintile of income in that city. When we use district of residence coupled with a broader indicator of deprivation (HDI) and a specific indicator for health deprivation (HNI), however, the picture changes significantly and the pro-neediest bias disappears. The percentage of individuals represented by the DP living in the lowest HDI districts and the highest HNI districts, arguably those whose need for healthcare is more urgent, falls to 49% and 42% respectively.
Differently from the cases represented by the DP, the class actions lodged by the MP are what we call structural cases, in the sense that they try to promote significant changes in the public health policies that will affect a larger number of people (improvement in public health units and inclusion of medicines or treatments in the public system), rather than seek a health benefit for a single individual.
Among the cases described in Section 3.2, the case in which free public transportation was demanded for low income pregnant women is the only one in which the lawsuit was clearly aimed at benefiting the poor. This makes the question we are trying to answer here a lot trickier than in the DP cases. Indeed, whether the poor or the severely poor are benefited by MP, right to health litigation is more difficult to answer in these structural cases in which a large-scale public policy that can potentially benefit a large group of individuals is at stake. More in depth research would be necessary to assess which social classes are more affected by these policies and who are the people who actually end up benefiting from these policies. This is crucial given that we can neither take for granted that these policies are effectively implemented nor that, when they are, they are extended to everyone who could potentially benefit (they might well be only “nominally universalized”, GAURI; BRINKS, 2008).
A good illustration of this is the civil action brought by the MP to force the state of São Paulo to provide all autistic individuals with special health care and education. Despite winning in the courts, the decision is far from being fully implemented several years after it was handed down. The obstacles, not surprisingly, are lack of sufficient resources, the need to hire staff and build new facilities, which takes time, and probably also some inefficiency and lack of political will. As a consequence, out of the hundreds of thousands of potential beneficiaries of the decision, only some of them are actually benefiting from it. Several hundred, it is noteworthy, with the help of private lawyers, who use the decision of the civil action sponsored by the MP to claim, almost always successfully, that the state should provide their individual client’s with a place in a private institution until it fully implements the decision.13
With the data we collected we cannot therefore answer these important questions for all civil actions sponsored by the MP, so we decided to focus our analysis on 22 cases in which the MP intended to force the government to improve the functioning of public health units (hospitals, primary care units and clinics). In such cases, through the location of these health units we are able to perform an analysis similar to the one made for the DP cases using HDI and HNI.
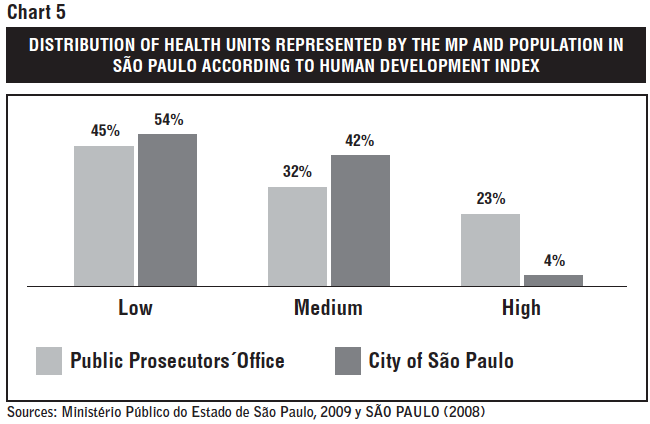
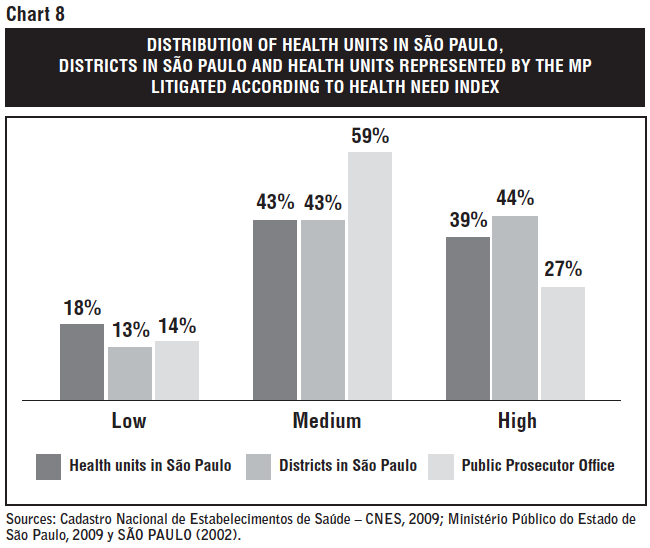
The first aspect to note is that, when concerned with improving health units (hospitals, clinics, etc.), the MP tends to bring more cases involving districts with a high HDI. Even though only 4% of the population in São Paulo live in districts that have high HDI, 23% of the cases lodged by the MP involve districts in this category (see Chart 8).
Yet districts with low HDI, although comprising 54% of the population, are involved in 45% of the MP lawsuits. Districts with a medium HDI, in which 42% of the population live, have filed comparatively fewer right to health lawsuits (32%) (see Chart 5).
The first hypothesis to explain this difference is that class actions are more difficult to lodge. Class actions do not depend simply on proving that one individual’s health need is unattended by the state. They demand more extensive work, requiring extensive evidence research and technical expertise. Consequently, health units in areas that are covered by the media and the public opinion and where users tend to have more education may be ahead of others in the competition for these resources.
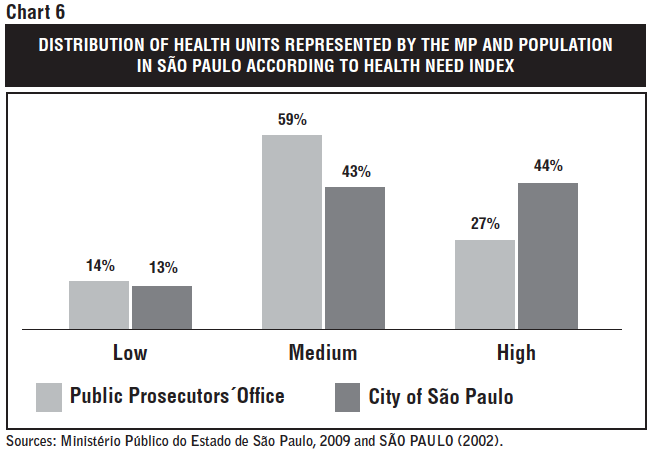
When we look at the Health Need Index, it is clear that districts with high levels of health needs receive the least attention from the Public Prosecutors’ Office (see Chart 6). These areas are arguably those in which the right to health requires more urgent protection. However, most lawsuits filed by the MP are in areas where the health needs are comparatively low. Even though 44% of the population in São Paulo lives in areas of high HNI, the MP directed to these districts only 27% of its right to health litigation (see Chart 6).
Again, this could happen due to the inequality in access to Justice, or more specifically, inequality to access to the attention from and representation of the Public Prosecutor’s Office, as was explained in the item above.
But one could also inquire whether this is not rather the consequence of the geographic inequality in the distribution of health services in São Paulo. Since the MP can obviously only sue health units where the health units are, it would not be surprising that litigation seeking the improvement of health units are concentrated in the comparatively more affluent areas if health units were mostly located there.
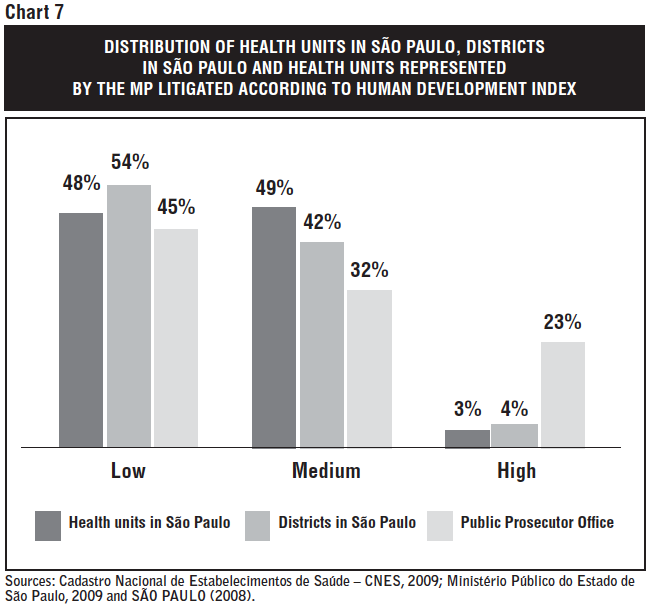
In order to test this hypothesis, and based on the National Survey of Health Units (Cadastro Nacional de Estabelecimentos de Saúde (CNES)), we listed all the 1,109 health units in São Paulo city14 and classified them according to the HNI and HDI of the districts where they are located. The result is that, in spite of some differences, the distribution of health units according to HDI and HNI is largely well balanced across districts (See Chart 7 and 8).
Thus, health units in areas where human development is low and health needs are high are less represented not because there are no or fewer health units there, but because they received, for some reason, less attention from the MP.
It is also interesting to note that among the 22 health units in which bad conditions were complained through a lawsuit lodged by the MP, only 3 of them were basic health units, whereas 9 were hospitals. Based on the fact that 55% percent of the health units in São Paulo are basic health units and only 9% are hospitals, we can affirm that the MP lawsuits are more focused on middle and high complexity healthcare rather than focused on preventive and basic healthcare.
The data presented above show some interesting patterns in right to health litigation sponsored by public lawyers in the city of São Paulo. For health litigation to be regarded as a positive tool in the implementation of the right to health in the non-neutral, pro-poor interpretation we adopt in this article, it must, at least, reverse two main characteristics that are currently prevalent in the so-called Brazilian model of right to health litigation: (a) it must be extended significantly beyond the narrow group of middle class and upper middle class individuals represented by private lawyers that currently dominate this type of litigation in São Paulo to include the most disadvantaged in society in terms of health needs (i.e. improve access to Justice) and (b) it must change its focus from new and expensive treatment to health actions and services that are a priority for these most disadvantaged groups, mostly primary care facilities and actions.
In this article we looked at the litigation record of the two institutions in Brazil that could potentially do this, the MP and DP, given that their remit is exactly to protect the public interest and the interests of the most disadvantaged.
As regards the first condition (enhancement of access to Justice to the most needy), we have used, where available, three different indicators of health disadvantage: income, human development, and health need. The first one (income) is collected through self-declaration and seems to indicate that the DP (no data is available for the MP) does represent mostly individuals who are poor and extremely poor in purely economic terms (varying from 80% to 88% depending on the year). However, when HDI or HNI are used, the picture seems to change. As regards the DP, only 49% of individuals represented come from districts with low human development, and only 42% come from districts with high health needs. That is, most DP litigation happens in districts that have medium and high human development (51%) and low and medium health needs (58%).
Two main hypotheses present themselves to interpret these apparently contradictory data concerning the profile of litigants represented by the DP. The first hypothesis is that household income is an indicator that should be taken with caution since this data is collected through self-declaration. Citizens may have underestimated their household income and declared it to be lower than the poverty threshold established by the DP in order to receive free legal aid. Moreover, research on the reliability of data on self-declared household income has shown that it tends to be systematically underestimated (COLLINS; WHITE, 1996; MICKLEWRIGHT; SCHNEPF, 2010). People may have imperfect information about the income of the other members of the house, and tend to leave out contributions from sources such as part-time earnings and social benefits.
The second hypothesis is that the DP is more accessible to individuals who are economically poor yet live in better areas. The fact that they live in more affluent areas possibly implies that they have more access to information concerning their rights and the existence of institutions providing free legal aid. Moreover, these people have better access to public services and facilities that make more probable that their unfulfilled health needs will lead to a lawsuit, such as a hospital from where they can get a medical prescription and public transportation to go the DP office.
Our data does not allow us to test which hypothesis is the correct one (maybe a combination of both is), but both seem to indicate that the DP finds obstacles to reach those in the most deprived areas of the city.
Moreover, access to health care litigation does not necessarily imply promotion of health equity. The object of litigation (our second condition) would also have to be of a transformative nature, that is, it would have to focus on health actions and services which are urgently needed by the most disadvantaged. This article was not able (for lack of space and data) to develop this aspect in much significant detail, yet the emerging data indicates that this condition is also far from being fulfilled. Most of the cases represented by the DP, are individual actions for items such as diapers and diabetes drugs. Even though these may be important for those who eventually receive health care by means of litigation, individual cases will seldom promote structural changes in the public health policies that may affect positively a larger share of the poor population.
It could be expected that the cases that demand structural changes – such as the MP class actions – would have greater potential to improve health services for the poor. Nonetheless, our research suggests that the MP actions are giving disproportionately more attention to those areas where the right to health is comparatively better fulfilled and not sufficiently focusing on basic and primary healthcare, the improvement of which is essential for an equitable health system (MEDICI, 2011). Only 27% of its lawsuits are filed in districts with high health needs and only 45% in districts with low human development.
Again, the bulk of litigation concentrates on districts with low and medium health needs and medium and high human development and on middle and high complexity healthcare rather than focused on preventive and basic healthcare. Moreover, we have seen that MP class actions rate of success in upper courts are lower when compared to individual lawsuits, which suggests that Courts are more prone to individual solutions rather than structural ones.
The empirical analysis of the socio-economic profile of litigants represented by public attorneys, the types of health benefits they claimed and the lower rate of success of collective cases involving structural changes indicate that even litigation sponsored by public attorneys face important obstacles for reaching the neediest.
Providing free legal representation does not in itself guarantee that the worst-off will be able to take their grievance to courts. As Felstiner, Abel, and Sarat (1980) have persuasively argued, there is a long process between a situation of personal distress or injustice that could potentially be judicially redressed and the start of a legal dispute. First, the person has to perceive that a particular experience has been injurious. Second, the injured person has to feel wronged and believe something might be done in response to the injury. Thirdly, the person has to transform his grievance into a claim against the person or entity believed to be responsible and ask for a remedy. Finally, if this claim is rejected, the person must have the knowledge and resources to resort to the next step: litigation. There is a long and complex way to be trodden, therefore, between suffering an injury and resorting to litigation, which is not accessible to a great number of individuals.
This analysis can explain some of the obstacles that seem to hinder the use of litigation in Brazil to benefit the worst-off. Considering that one of the main problems in the Brazilian healthcare system is the inequality in the access to basic and preventive health (MEDICI, 2011), and that education and information are important determinants of access to health care (SANCHEZ; CICONNELI, 2012), many poor people are not even aware of their health problems – especially when it comes to chronic diseases – or may just realize it when it is too late. Among those who know that they have a health problem, just the better educated and informed will know that they could be receiving treatment from the public health service as a matter of constitutional right. And not all of them will know that if they are refused treatment, they can make a claim against government. Finally, only a small number of people will know that there are public institutions that provide free legal aid, such as the DP and the MP.
It is hardly surprising, then, that the Brazilian model of litigation, where cases brought by comparatively better off individuals represented by private lawyers, prevails in most places around the country, and that even litigation sponsored by public attorneys can face important obstacles to depart significantly from that model.
1. There is no comprehensive study as yet that shows the precise volume of litigation across the country. Octavio Ferraz has arrived at 40.000 cases per year in a conservative estimate done through several different studies (FERRAZ, 2011a).
2. For a clear example of this polarization see the debate between the pro-litigation lawyers Andrea Lazzarini Salazar and Karina Bozola Grou (“As Verdadeiras Causas e Consequências”, Folha de S. Paulo, 9 maio 2009) and the public health expert, against litigation, Marcos Bosi Ferraz. (“O STF e os Dilemas da Saúde”, Folha S. Paulo, 9 maio 2009). An example of an academic defense of litigation can be found in (PIOVESAN, 2008).
3. One of the hypothesis to explain the high rate of litigants represented by public attorneys in Rio de Janeiro and Rio Grande do Sul is that, in the former state, the income threshold to receive legal aid from the Public Defensory is higher than in other states (PEPE et al., 2010) and, in the latter, there is not an income threshold and the need of the patient will be assessed in each case based on a questionnaire, provision of documents and self-declaration (see Rio Grande do Sul Public Defensory Office official website http://www.dpe.rs.gov.br/site/faq.php. Last accessed on: May 2013)
4. There is also the possibility that NGOs, in particular patient’s associations, bring collective claims on behalf of groups of needy patients, and/or finance individual litigation, which could promote access to Justice for disadvantaged groups. We have not looked at this type of litigation in our study. We are however confident that the potential transformative impact of such litigation is not as great as that sponsored by public attorneys. There have been studies that show that some NGOs have indeed sponsored patient’s litigation, yet on an individual basis, and often for a particular disease and focused mainly on certain expensive drugs (SILVA; TERRAZAS, 2011). There are also studies that suggest a link between these patient’s associations and the pharmaceutical industry. (CHIEFFI; BARATA, 2010).
5. SÃO PAULO (Estado), 2006.
6. BRASIL, 1988, Article 129, II and III.
7. Note however that this is not a rigid rule, and thus one can find both collective lawsuits being filed by the DP and individual ones being brought by the MP (Interview with the Public Defendants Rafael Vernaschi, Vania Casal and Sabrina Carvalho in 29 July of 2009).
8. In these cases there were only general complaints about the lack of medicines, not specifying which drugs were lacking.
9. That is why in many cases there is no information on how many members there are in each family. Yet this data appears in some cases to explain why someone whose family income was above the threshold was still able to receive legal assistance from the DP due to the large size of his or her family.
10. The data on HNI and HDI in São Paulo city was calculated based on studies published by the São Paulo Secretary of Health (SÃO PAULO, 2008) and the São Paulo Secretary of Development Work and Solidarity (SÃO PAULO, 2002), respectively.
11. We are also aware that one has to be careful when using district level information as a proxy to individual characteristics because districts can be internally unequal (some areas in the same district can be better than others) and people with different socioeconomic backgrounds can live very close to each other. However, we consider that district is a good (although imperfect) proxy to measure someone’s socioeconomic condition. A district HDI and HNI performance is partially caused by reasons that are geographically determined, for example, access to education, basic sanitation, healthcare facilities and other public services. And access to these services, which is geographically distributed, can impact on individuals’ level of deprivation.
12. It is important to remark that the proportion of poor and extremely poor people in our analysis is possibly underestimated. It is known that poor families usually have more members than the average (3.2 people per family). However, because we do not have more accurate numbers, the average should be used.
13. Interview with Public Attorney’s (2011).
14. The National Survey of Health Units is available in http://www.saude.sp.gov.br/ses/perfil/cidadao/homepage/destaques/unidades-de-saude. Last accessed on: May 2013.
Bibliography and other sources
BIEHL, João et al. 2012. Between the court and the clinic: Lawsuits for medicines and the right to health in Brazil. Health and Human Rights: an international journal, v. 14, no. 1, p. 36-52, June.
BRASIL. 1988. Constituição (1988). Constituição da República Federativa do Brasil. Brasília, DF: Senado Federal, 1988.
______. 2010a. Superior Tribunal Federal. Suspensão de Tutela Antecipada STA 424 SC. Available at: http://stf.jusbrasil.com.br/jurisprudencia/19133128/suspensao-de-tutela-antecipada-sta-424-sc-stf. Last accessed: May 2013.
______. 2010b. Superior Tribunal Federal. Suspensão de Liminar SL 256 TO. Available at: http://stf.jusbrasil.com.br/jurisprudencia/9087208/suspensao-de-liminar-sl-256-to-stf. Last accessed: May 2013.
CHIEFFI, Ana Luiza; BARATA, Rita Barradas. 2009. Judicialização da política pública de assistência farmacêutica e equidade. Cadernos de Saúde Pública, Rio de Janeiro, v. 25, n. 8, p. 1839-1849, ago.
______. 2010. Ações judiciais: estratégia da indústria farmacêutica para introdução de novos medicamentos. Revista de Saúde Pública, v. 44, no. 3, p. 421-429.
COLLINS, Debbie.; WHITE, Amanda. 1996. In search of an income question for the 2001 Census. Survey Methodology Bulletin, v. 39, no. 7, p. 2-10, July.
DIEESE. 2009. Relação família e trabalho na perspectiva de gênero: a inserção de chefes e cônjuges no mercado de trabalho. Estudos Especiais. Available at: http://www.seade.gov.br/produtos/mulher/boletins/anexo_mtrabalho_chefesconjuges.pdf. Last accessed on: May 2013
EPP, Charles R. 1998. The rights revolution: lawyers, activists and supreme court in comparative perspective. Chicago; London: The University of Chicago Press.
FERRAZ, Octavio Luiz Motta. 2009. The right to health in the courts of Brazil: worsening health inequities? Health and Human Rights: an international journal, v. 11, no. 2, p. 33-45.
______. 2011a. Brazil. Health inequalities, rights and courts: the social impact of the “judicialization of health” in Brazil. In: YAMIN, Alicia Ely; GLOPPEN, Siri (Eds.). Litigating health rights: can courts bring more justice to health systems? Cambridge, MA: Harvard University Press.
_______. 2011b. Harming the poor through social rights litigation; lessons from Brazil. Texas Law Review, v. 89, no. 7, p. 1643-1668.
FERRAZ, Octavio Luiz Motta; VIEIRA, Fabiola Sulpino. 2009, The right to health, scarce resources, and equity: inherent risks in the predominant legal interpretation (in portuguese: Direito à saúde, recursos escassos e equidade: os riscos da interpretação judicial dominante). Dados, Rio de Janeiro, v. 52, no. 1, p. 223-251.
GARGARELLA, Roberto; DOMINGO, Pilar; ROUX, Theunis (Eds.). 2006. Courts and social transformation in new democracies: an institutional voice for the poor? Hampshire, England; Burlington, VT: Ashgate.
GAURI, Varun; BRINKS, Daniel M. (Eds.). 2008. Courting social justice: judicial enforcement of social and economic rights in the developing world. Cambridge; New York: Cambridge University Press.
LADERCHI, Caterina Ruggeri; SAITH, Ruhi; STEWART, Frances. 2003. Does it matter that we do not agree on the definition of poverty?: a comparison of four approaches. Oxford Development Studies, v. 31, no. 3, p. 243-274.
MACEDO, Eloisa Israel de; LOPES, Luciane Cruz; BARBERATO-FILHO, Silvio. 2011. A technical analysis of medicines request-related decision making in Brazilian courts. Revista de Saúde Pública, v. 45, no. 4, p. 706-713, Aug.
MACHADO, Marina Amaral de Ávila et al. 2011. Judicialization of access to medicines in Minas Gerais State, Southeastern Brazil. Revista de Saúde Pública, São Paulo, v. 45, no. 3, p. 590-598, June.
MAESTAD, Ottar; RAKNER Lise; FERRAZ, Octavio Luiz Motta. 2011. Assessing the impact of health rights litigation: a comparative analysis of Argentina, Brazil, Colombia, Costa Rica, India and South Africa. In: YAMIN, Alicia Ely; GLOPPEN, Siri (Eds.). Litigating the right to health: can courts bring more justice to health? Cambridge, MA: Harvard University Press.
MÉDICI, André Cezar. 2011. Propostas para melhorar a cobertura, a eficiência e a qualidade no setor saúde. In: BACHA, Edmar Lisboa; SCHWARTZMAN, Simon (Orgs.). Brasil: a nova agenda social. Rio de Janeiro: LTC; IEPE/CDG. p. 23-93.
MESSEDER, Ana Márcia; OSORIO-DE-CASTRO, Claudia Garcia Serpa; LUIZA, Vera Lucia. 2005. Mandados judiciais como ferramentas para garantia do acesso a medicamentos no setor público: a experiência do Estado do Rio de Janeiro, Brasil. Cadernos de Saúde Pública, v. 21, n. 2, p. 525-534, mar./abr.
MICKLEWRIGHT, John; SCHNEPF, Sylke Viola. 2010. How reliable are income collected with a single question? Journal of the Royal Statistical Sociery, v. 173, no. 2, p. 409-429.
NORHEIM, Ole Frithjof; GLOPPEN, Siri. 2011. Litigating for medicines: How can we assess impact on health outcomes? In: YAMIN, Alicia Ely; GLOPPEN, Siri (Eds.). Litigating health rights: can courts bring more justice to health. Cambridge, MA: Human Rights Program, Harvard Law School; Harvard University Press. p. 304-330.
PEPE, Vera Lucia Edais et al. 2010. Characterization of lawsuits for the supply of “essential” medicines in the State of Rio de Janeiro, Brazil. Cadernos de Saúde Pública, v. 26, no. 3, p. 461-471, Mar.
PEREIRA, Januária Ramos et al. 2010. Situation of lawsuits concerning the access to medical products by the Health Department of Santa Catarina State, Brazil, during the years 2003 and 2004. Ciência & Saúde Coletiva, v. 15, no. 3, p. 3.551-3.560.
PIOVESAN, Flavia. 2008. Brazil: impact and challenges of social rights in the courts. In: LANGFORD, Malcolm. (Ed.). Social rights jurisprudence: emerging trends in international and comparative law. Cambridge: Cambridge University Press. p. 182-191.
ROCHA, Sonia. 2009. Pobreza e indigência. Instituto de Estudos do Trabalho e Sociedade (IETS). Available at: http://www.iets.org.br/article.php3?id_article=915. Last accessed on: May 2013.
SANCHEZ, Raquel Maia; CICONELLI, Rozana Mesquita. 2012. Conceitos de acesso à saúde. Revista Panamericana de Salud Pública, Washington, v. 31, n. 3, p. 260-268, mar.
SANT’ANA, João Maurício Brambati. 2009. Essencialidade e assistência farmacêutica: um estudo exploratório das demandas judiciais individuais para acesso a medicamentos no Estado do Rio de Janeiro. Dissertação (Mestrado) – Escola Nacional de Saúde Pública Sergio Arouca, Rio de Janeiro.
SANTOS, Carla Carlos do. 2006. Estratégias para reorganização e otimização das atividades destinadas ao fornecimento de medicamentos demandados judicialmente contra a Secretaria de Estado de Saúde do Distrito Federal. Dissertação (Mestrado) – Universidade de Brasília, Brasília.
SÃO PAULO (Cidade). 2002. Prefeitura do Município de São Paulo. Secretaria do Desenvolvimento, Trabalho e Solidariedade, São Paulo. Desigualdade em São Paulo: o IDH.
______. 2008. Prefeitura do Município de São Paulo. Secretaria Municipal da Saúde. Coordenação de Epidemiologia e Informação (CEInfo). Índice de Necessidades em Saúde por Distrito Administrativo do Município de São Paulo – 3ª edição (junho/2008). Available at: http://extranet.saude.prefeitura.sp.gov.br/areas/ceinfo/INS_3edicao_Junho2008.pdf. Last accessed on: May 2013
SÃO PAULO (Estado). 2006. Lei Complementar Nº 988. Organiza a Defensoria Pública do Estado, institui o regime jurídico da carreira de Defensor Público do Estado. 9 de janeiro de 2006. Available at: http://www.defensoria.sp.gov.br/dpesp/Default.aspx?idPagina=2939. Last accessed on: May 2013.
SCHEFFER, Mário; SALAZAR, Andréa Lazzarini; GROU, Karina Bozola. 2005. O remédio via Justiça: um estudo sobre o acesso a novos medicamentos e exames em HIV/AIDS no Brasil por meio de ações judiciais. Brasília: Ministério da Saúde, Secretaria de Vigilância em Saúde, Programa Nacional de DST e Aids.
SEN, Amartya. 1992. Inequality reexamined. Oxford: Clarendon Press.
TAYLOR, Matthew M. 2006. Beyond judicial reform: courts as political actors in Latin America. Latin American Research Review, v. 41, n. 2, p. 269-280.
VIEIRA, Fabíola S.; ZUCCHI, Paola. 2007. Distorções causadas pelas ações judiciais à política de medicamentos no Brasil. Revista de Saúde Pública, São Paulo, v. 41, n. 2, p. 214-222.
WANG, Daniel Wei Liang; TERRAZAS, Fernanda; CHIEFFI, Ana Luiza. 2012. Public system responses to right to health litigation: the case of the State of São Paulo Secretary of Health. Annual Meeting of the Law and Society Association, 03 Jun. 2012, Honolulu, HI.

