
The fantasy of “foreigners carrying disease” justifies measures that restrict international migration and foster human rights violations
This article offers an overview of the impact of health crises on the rights of migrants. It demonstrates that the repercussions of the Ebola crisis on human mobility is not a novelty. The association between foreigners and disease accompanies the history of epidemics and is part of the process of constructing national identities in the West, which maintains the potential for inciting or justifying human rights violations. Deisy Ventura argues that the restrictions on international migration adopted during the Ebola crisis are illegal under international health law and counterproductive to the effort to combat the epidemic. Furthermore, the she considers the security-based approach to international migration and health to be the seed of a kind of totalitarian utopia - it spreads the illusion that only surveillance systems are capable of preventing disease from propagating internationally, without, however, guaranteeing the right to health in all regions of the world. Finally, Ventura invites readers to look at the interface between the health crisis and international migration through the prism of the debates that animate the field of global health.
In 2014, at the peak of the Ebola epidemic in West Africa, various countries, including Australia and Canada, restricted the entry of people into their territory from the countries affected the most by the disease (Guinea, Liberia and Sierra Leone).11. Reena Pattani, “Unsanctioned Travel Restrictions Related To Ebola Unravel The Global Social Contract,” Canadian Medical Association Journal 187, no. 3 (2015):166-167, accessed May 8, 2016, http://www.cmaj.ca/content/187/3/166.full. Large airline companies, such as British Airways and Emirates Airlines, suspended part or all of their flights to the affected region.22. Mark Anderson, “Ebola: Airlines Cancel More Flights To Affected Countries.” The Guardian, Aug. 22, 2014, accessed May 8, 2016, http://www.theguardian.com/society/2014/aug/22/ebola-airlines-cancel-flights-guinea-liberia-sierra-leone. Void of plausible scientific or public health justifications, these measures ignored the World Health Organisation’s (WHO) strong statement against the adoption of travel restrictions, except for people with the disease and those in direct contact with them, as such restrictions would obstruct the arrival of aid to the most affected countries, among other reasons.33. See: “Statement on the 2nd meeting of the IHR Emergency Committee Regarding the 2014 Ebola Outbreak in West Africa,” OMS, Sept. 22, 2014, accessed May 8, 2016, http://www.who.int/mediacentre/news/statements/2014/ebola-2nd-ihr-meeting/en/. The countries adjacent to the epicentre of the crisis closed their borders. In the case of the Ivory Coast, for example, this measure prevented thousands of Ivorian refugees in Liberia from returning to their country.44. Alexis Adele, “A Long Wait For Home - How Ebola Kept Refugees Stuck In Liberia.” IRIN News, Mar. 18, 2015, accessed May 8, 2016, https://www.irinnews.org/analysis/2015/03/18-0. Repatriation began again at the end of 2015. See: “Ivorian Returns Resume From Liberia After Ebola Outbreak,” UNHCR, December 18, 2015, accessed May 8, 2016, http://www.unhcr.org/5674384d6.html.
In addition to restricting human mobility, the Ebola crisis caused an increase in discrimination against black migrants, including those from regions where the disease did not exist, as, for instance, in the case of Haitians in Brazil.55. A study by Denise Cogo and Terezinha Silva concluded that among the seven main events and issues related to Haitian immigration in Brazil covered by the media between 2010 and 2014, one finds the "international Ebola epidemic, brought up in mid-2014 in coverage on daily situations where Haitians were suspected (of having Ebola) or discriminated against in Brazilian cities". See Denise Cogo and Terezinha Silva, “Entre a Fuga e a Invasão: Alteridade e Cidadania da Imigração Haitiana na Mídia Brasileira,” Revista Famecos - Mídia, Cultura e Tecnologia 23, no.1 (2016), accessed May 8, 2016, http://revistaseletronicas.pucrs.br/ojs/index.php/revistafamecos/article/view/21885. At the same time, the adoption of discriminatory measures towards health professionals who had worked in West Africa upon their return to their respective countries of origin, such as Spain, the United States of America (U.S.) and the United Kingdom,66. See, for example, the account of U.S. doctor Craig Spencer, “Having and Fighting Ebola - Public Health Lessons from a Clinician Turned Patient,” New England Journal of Medicine 372 (2015) :1089-1091 accessed May 8, 2016, http://www.nejm.org/doi/full/10.1056/NEJMp1501355. was denounced. The privacy of patients or suspected cases, including migrants or refugees, was unnecessarily violated in many cases.77. In Brazil, the identity of one person suspected of having the disease and who was applying for refugee status was disseminated widely. See Deisy Ventura and Vivian Holzhacker, “Emergências Internacionais de Saúde Pública e Direitos Humanos: O Primeiro Caso Suspeito de Ebola no Brasil”, Lua Nova, no. 98.
This article seeks to identify, generally and briefly, the impact of health crises on the rights of migrants. The first section demonstrates that the repercussions of the Ebola crisis on human mobility is not something new. The association between foreigners and disease accompanies the history of epidemics and is part of the process of constructing national identities in the West. It is maintained so it can be potentially used to induce or justify human rights violations. The second section argues that the restrictions on international migration adopted during the Ebola crisis are illegal under international health law and counterproductive to the effort to combat the epidemic. Third, the article examines how the strengthening of a security-based approach to international migration and health is constructing a kind of totalitarian utopia, as it spreads the illusion that only surveillance systems are capable of preventing disease from propagating internationally. Finally, the conclusion invites readers to look at the interface between the health crisis and international migration through the prism of the conflicts that inflame the field of global health.
In his studies on the history of fear in the West between the 14th and the 18th centuries, Jean Delumeau elaborates a typology of collective behaviours during the great plague. He concludes that when confronted with an epidemic, the first and natural impulse, on both the individual and collective level, is to identify who is to blame as a way of making the apparently unexplainable explainable. Thus:
the ones who are potentially to blame, against whom the collective can turn its aggression, are first the foreigners, travellers, marginalised and all those who are not well integrated into a community, either because they do not want to accept their beliefs – in the case of the Jews – or because it was necessary to expel them to the edge of the group for obvious reasons – such as the lepers – or simply because they are from somewhere else and, as such, they are somewhat suspicious.88. Jean Delumeau, La Peur en Occident (XIVe-XVIIIe siècles) - Une cité assiégée (Paris: Fayard, 1978): 131. The author offers numerous examples of how foreigners were held responsible for the Black Death: in Lorena, in 1627, the plague was called the "Hungarian Plague" and in 1636, "Swedish"; in 1630 in Toulouse, the "Plague of Milan"; in Cyprus, Christians massacred Muslim slaves; in Russia, the Tatars were attacked; in 1665, the British accused the Dutch, etc.
The rejection of foreigners in general is based on a “vulgar synthesis of incomplete information” that forges “naively schematic” collective stereotypes capable of “haunting the popular imagination”.99. Charles-Victor Langlois, “Les Anglais du Moyen Âge d’Après les Sources Françaises,” Revue Historique t. 52, fasc. 2 (1893): 298-315. In the Middle Ages, a particular kind of xenophobia founded on cultural and political reasons rejected Saracens and Byzantines. This contributed to the development of a Westerner identity in opposition to “Easterners”. Later, discrimination towards Iberians and Italians ended up highlighting the difference between political regimes, as part of the idealisation of the figures of the Western man and the French monarchy.1010. Franck Collard, “Une Arme Venue D’ailleurs. Portrait De L’étranger En Empoisonneur,” Actes des Congrès de la Société des Historiens Médiévistes de l’Enseignement Supérieur Public 30, no. 1 (1999): 95-106, accessed May 8, 2016, http://www.persee.fr/doc/shmes_1261-9078_2000_act_30_1_1762. Therefore, throughout history, the examples of identities whose foundations are based on repulsion towards foreigners corroborates the idea that “foreigners do not exist as such; one is only foreign before a norm, a culture or a civilisation. In sum, foreigners only exist in relation to the other”.1111. Bernard Cottret, Terre d’Exil. L’Angleterre et Ses Réfugiés Français et Wallons, de la Réforme à la Révocation de l’Édit de Nantes, 1550-1700 (Paris: Aubier, 1985): 55-56.
This very brief historical overview confirms the modern idea that any attempt to “rationally calculate” the risk of contracting a disease must face an imaginary woven together by various representations1212. Delphine Moreau, “Dispositifs de Sécurité et Épidémie de SIDA”, Labyrinthe 22, no. 3 (2005), accessed May 8, 2016, http://labyrinthe.revues.org/1038. that includes both the popular view of immigrants as vectors of disease and the discourse of specialists who point to the epidemiological consequences of the migration of populations.1313. Didier Fassin, “L’Alterité de l’Épidemie. Les Politiques du SIDA à l’Épreuve de l’Immigration,” Revue Européenne des Migrations Internationales, 17, no. 2 (2001): 139-151, accessed June 1, 2016, http://www.persee.fr/doc/remi_0765-0752_2001_num_17_2_1782. A milestone in the history of global health, the HIV/AIDS epidemic that erupted in the 1980s resuscitated the archaic fears from major epidemics such as the plague and syphilis and, with them, more repressive means of protection targeted primarily the most stigmatised groups, such as homosexuals, drug users, prostitutes and foreigners.1414. Moreau, “L’Alterité de l’Épidemie,” 2001. In a study on the response to HIV/AIDS in China, Évelyne Micollier reveals that the “social construction of the disease”, especially in prevention campaigns, is built around the notion of the “foreigner” who carries the risk of contamination. In this notion, the Chinese include not only nationals from other states, but also Chinese people who are not from the Han ethnic group.1515. Evelyne Micollier, “L’Autre: Porteur Originel et/ou Vecteur Privilégié du VIH/SIDA (Chine Populaire-Taiwan),” Autrepart - Revue de Sciences Sociales au Sud (1999): 73-86, accessed May 8, 2016, http://hal.ird.fr/ird-00445745/document.
In the West, a myth emerged that accuses Haitians of being responsible for the origin and the spread of the HIV/AIDS epidemic in the U.S. The myth was fed by the theory on the risk groups known as the “4H”: haemophiliacs, Haitians, homosexuals and heroin addicts.1616. Also referred to as the "5H" when prostitutes (Hookers) are added. In a fundamental work on this issue, Paul Farmer demonstrated that this myth constitutes a process of “holding ethnic groups responsible” in which “the victims are blamed”. This process can only be understood when one takes into account the relations of political, social and economic domination between Haiti and the U.S.1717. Paul Farmer, AIDS and Accusation - Haiti and the Geography of Blame, 2a ed. (Berkeley: University of California Press, 2006). Farmer also refers to the occasional reversal of the accusatory discourse, as Haitians sometimes blame the United States for introducing HIV/AIDS into Haiti. However, various episodes illustrate the force of this amalgam. In 1993, the Senate banned the immigration of people living with HIV/AIDS, with the support of 71% of the U.S. population. This was in direct response to the 219 Haitian political refugees with HIV/AIDS who had been awaiting authorisation to enter the U.S. for nearly a year in the Guantanamo Bay naval base (Cuba).1818. “Près de Trois Quarts des Américains S’opposent à L’entrée Aus États-Unis des Étrangers Séropositifs,” Le Monde, Feb. 16, 1993, accessed May 8, 2016, http://www.lemonde.fr/archives/article/1993/02/16/pres-de-trois-quarts-des-americains-s-opposent-a-l-entree-aux-etats-unis-des-etrangers-seropositifs_3916822_1819218.html; and “Le Sénat Américain Interdit L’immigration des Étrangers Contaminés par le Virus du SIDA,” Le Monde, Feb. 20, 1993, accessed May 8, 2016, http://www.lemonde.fr/archives/article/1993/02/20/reperes-medecine-le-senat-americain-interdit-l-immigration-des-etrangers-contamines-par-le-virus-du-sida_3918279_1819218.html.
Moving on to modern day Brazil, a case study on Haitian migration in Tabatinga (in the state of Amazonas) revealed that “health was undoubtedly the principle element crystallising the fear the Haitian migrants inspired in the local population”. This fear was fed by the idea – promoted mainly by city councillors and the local media – that this “uncontrolled and dangerous” wave of migration would bring major health risks to the area.1919. Jean-François Veran et al., “Nem Refugiados, Nem Migrantes: A Chegada dos Haitianos à Cidade de Tabatinga (Amazonas),” Dados 57, no. 4 (2014): 1007-1041, accessed May 8, 2016, http://dx.doi.org/10.1590/00115258201431. However, the authors noted that this alarmism is contrary to reality, as the Doctors Without Borders team that assessed the migrants’ health considered that their general state of health was no different from that of the local population.
The repercussions of the international Ebola crisis in Brazil made fears grow in spite the fact that no cases have been reported in the country. One must understand that the disease is not what gave rise to stigmatisation of foreigners: on the contrary, it came to fill the opening for rejection that already existed.2020. Didier Fassin, “Une Double Peine - La Condition Sociale des Immigrés Malades du SIDA,” L’Homme, no. 160 (2001): 137-162. This is what the study of the media coverage on the Ebola crisis in Brazil revealed: it noted that the coverage reinforced the idea that Africa is a place full of health risks and Africans are agents that disseminate Ebola, thereby promoting and constructing “Africanness as a risk factor for health”.2121. Igor Sacramento and Izamara Machado, “A Imigração Como Risco Para a Saúde: Uma Análise das Representações do Imigrante Africano na Cobertura da Folha de S. Paulo Sobre o Ébola,” Comunicação e Sociedade (Portugal) 28 (2015): 25-47.
However, the coverage of the Ebola crisis by the Brazilian press is not an exception, but rather the rule. The seven Ebola cases reported in the West (four in the U.S. and single cases in Spain, Italy and the United Kingdom), of which only one resulted in death, had much greater repercussions than the thousands of cases and deaths that occurred in Guinea, Liberia and Sierra Leone.2222. Deisy Ventura, “From Ebola to Zika: international emergencies and the securitization of global health,” Cadernos de Saúde Pública 32, no. 4 (2016): e00033316, accessed May 8, 2016, http://www.scielo.br/pdf/csp/v32n4/en_1678-4464-csp-32-04-e00033316.pdf. As of 5 May 2016, the WHO had been notified of a total of 28,616 confirmed, probable or suspected cases and 11,310 deaths.2323. “Ebola Situation Report,” OMS, May 5, 2016, accessed May 8, 2016, http://apps.who.int/iris/bitstream/10665/205945/1/ebolasitrep_5may2016_eng.pdf?ua=1. Prior to the Ebola virus being declared as a Public Health Emergency of International Concern (PHEIC) by the WHO in August 2014,2424. Statement on the 1st Meeting of the IHR Emergency Committee on the 2014 Ebola Outbreak in West Africa,” WHO, Aug. 8, 2014, accessed May 8, 2016, http://www.who.int/mediacentre/news/statements/2014/ebola-20140808/en/. outbreaks of diseases in Africa had received little attention since the 1970s. No matter how dangerous a virus may be, if it does not generate a significant market – which was the case of the Ebola virus – it tends to be neglected. This explains the absence of treatments and vaccines when an epidemic breaks out. However, “the market appears when the virus leaves a country where the West really wants it to stay”.2525. Bruno Canard, “Ebola: La Terreur Utile.” Le Monde, Aug. 13, 2014, accessed May 8, 2016, http://www.lemonde.fr/idees/article/2014/08/13/ebola-la-terreur-utile_4471002_3232.html#SjZtw67C4QLYFD1A.99.
The economic determinants of the seriousness of a disease supports, in a way, the idea that “health means having the same diseases as our neighbours”.2626. Quentin Crisp, The Naked Civil Servant (New York: Penguin, 1997). The reaction of a part of the political class and media in the U.S., which was opposed to the repatriation of U.S. health professionals who had worked to fight the Ebola virus, at the height of the crisis, appears to reflect such a view. The previous rejection of these professionals was probably due to the fact that they “were where they shouldn’t be” – that is, they did not go along with the general indifference towards the health of the majority of the world population so that the enormous distortions in the current global health governance could be maintained.2727. On the global governance of health and inequalities, see Dominique Kerouedan and Joseph Brunet-Jailly (Orgs.), Santé Mondiale. Enjeu Stratégique, Jeux Diplomatiques (Paris: Presses de Sciences Po, 2016); and Ottersen et al., “The political origins of health inequity: prospects for change.” Commission Report The Lancet - University of Oslo, February 2014, accessed May 8, 2016, http://www.thelancet.com/pdfs/journals/lancet/PIIS0140-6736(13)62407-1.pdf. During the campaign for mid-term elections in the U.S.,2828. Midterm elections are held to renew the entire US House of Representatives and a third of the Senate two years after presidential elections are held. some candidates resolved to exploit the health crisis politically.2929. Gregg Gonsalves and Peter Staley, "Panic, Paranoia and Public Health - The AIDS Epidemic’s Lessons for Ebola," New England Journal of Medicine 371 (2014): 2348-2349, accessed May 8, 2016, http://www.nejm.org/doi/full/10.1056/NEJMp1413425. Republican Donald Trump strongly attacked the Obama administration, arguing that “the U.S. cannot allow Ebola infected people back. People that go to far away places to help out are great-but must suffer the consequences!”3030. Donald Trump, Post do Twitter, Aug. 1, 2014, 6:22 p.m., accessed May 8, 2016, https://twitter.com/realdonaldtrump/status/495379061972410369.
The following series of cartoons by Patrick Chappatte, the rights for which were granted for free to this publication, is of great value to understand some elements of the complex impact of Ebola in the West.
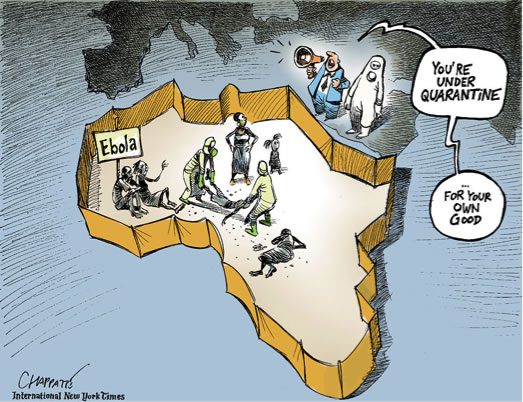 Figure 1 – Dealing With Ebola3131. Ebola is spreading © Chappatte in The International New York Times, August 27, 2014 (I140827).
Figure 1 – Dealing With Ebola3131. Ebola is spreading © Chappatte in The International New York Times, August 27, 2014 (I140827).
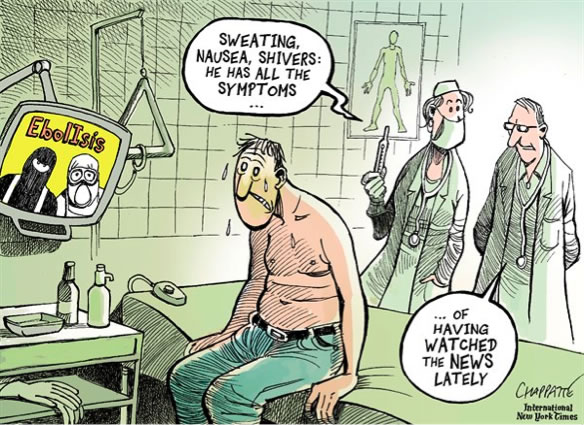 Figure 2 – Could it be Ebola? 3232. Ebol-ISIS: a scary world © Chappatte in The International New York Times, Oct 11, 2014 (I141011).
Figure 2 – Could it be Ebola? 3232. Ebol-ISIS: a scary world © Chappatte in The International New York Times, Oct 11, 2014 (I141011).
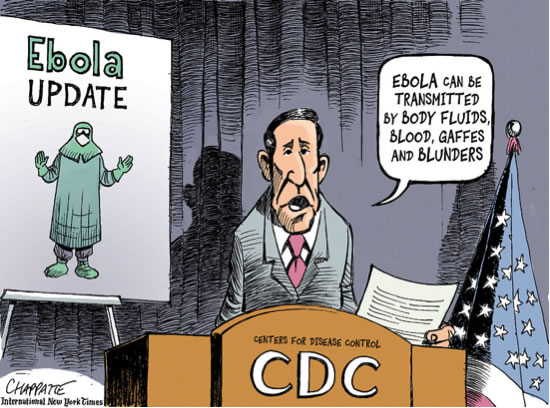 Figure 3 – The CDC’s Ebola Update3333. Ebola in the USA © Chappatte in The International New York Times, Oct 18, 2014 (I141018).
Figure 3 – The CDC’s Ebola Update3333. Ebola in the USA © Chappatte in The International New York Times, Oct 18, 2014 (I141018).
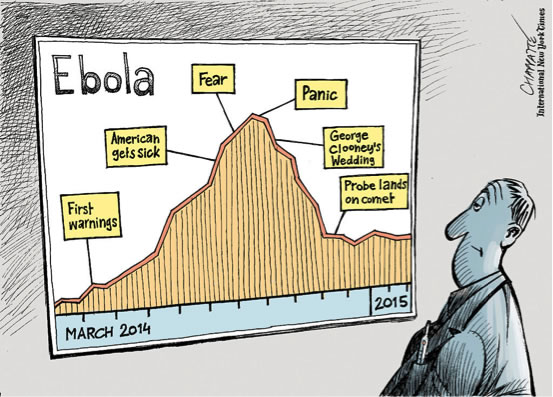 Figure 4 – The Year for Ebola3434. The Year of Ebola © Chappatte in The International New York Times, March 25, 2015 (I150325).
Figure 4 – The Year for Ebola3434. The Year of Ebola © Chappatte in The International New York Times, March 25, 2015 (I150325).
In sum, in the epicentre of the Ebola epidemic, it is unanimous that the international response to this neglected disease was deficient.3535. See, for example, Mit Philips and Áine Markham, “Ebola: A Failure of International Collective Action,” The Lancet 384, no. 9944 (2014): 637, accessed May 8, 2016, http://dx.doi.org/10.1016/S0140-6736(14)61377-5. Outside of the epicentre, paradoxically, the disease became exacerbated by a narrative that weaves together notions of security and crisis, sustained by a political and media spectacle.3636. João Nunes, “Ebola and the Production of Neglect in Global Health,” Third World Quarterly 37, no. 3 (2016): 542-556, accessed May 8, 2016, http://www.tandfonline.com/doi/full/10.1080/01436597.2015.1124724. However, the potential impact of this drama on human rights reached the justice system. The ruling on the unusual restrictions imposed by the government of the state of Maine on a U.S. nurse sent home from West Africa merits special attention. One of the restrictions was the order for her to maintain one metre of distance between herself and other people.3737. “State of Maine Department of Health and Human Services v. Kaci Hickox, Docket n. CV-2014-36, Order Pending Hearing," State of Maine, District Court - Fort Kent, Oct. 31, 2014, accessed May 8, 2016, http://www.courts.maine.gov/news_reference/high_profile/hickox/order_pending_hearing.pdf (p. 3). Even though the judge recognised the lack of scientific basis for his ruling, he based his decision on the recognition that people are acting out of fear and whether that fear is rational or not, “it is present and it is real”.
During the Ebola crisis, pressured by the panic that was spreading at a dizzying speed, more than 40 states did not abide by the WHO’s recommendations on human travel and trade. Few countries notified the WHO of the measures they adopted and some of them did not even answer the organisation when it questioned them about it. 3838. “Report of the Ebola Interim Assessment Panel,” OMS, July, 2015, accessed May 8, 2016, http://www.who.int/csr/resources/publications/ebola/report-by-panel.pdf. This led David Fidler to identify another epidemic: that of the non-compliance with norms, especially the International Health Regulations (IHR).3939. D. P. Fidler, “The Ebola Outbreak and the Future of Global Health Security,” The Lancet 385, no. 9980 (2015):1884-1901. In force in 196 countries, the IHR stipulate that prevention and the response to the international spread of disease is to be commensurate with risks and avoid unnecessary interference with international traffic and trade (Article 2), and will guarantee “full respect for the dignity, human rights and fundamental freedoms of persons” (Article 3).4040. Version in Portuguese approved by the National Congress, Legislative Decree 395/2009: OMS, Regulamento Sanitário Internacional OMS (Brasília: ANVISA, 2009), accessed May 8, 2016, http://portal.anvisa.gov.br/wps/wcm/connect/fe029a0047457f438b08df3fbc4c6735/Regulamento+Sanitario+Internacional+versao+para+impressao+090810.pdf?MOD=AJPERES. English version available at http://www.who.int/ihr/IHR_2005_en.pdf. According to Article 42 of the regulations, all measures must be adopted in a transparent and non-discriminatory manner.
In the opinion of Khalid Koser,4141. Khalid Koser, “Why Travel Bans Will Not Stop the Spread of Ebola.” World Economic Forum, Nov. 14, 2015, accessed May 8, 2016, https://www.weforum.org/agenda/2014/11/why-travel-bans-will-not-stop-the-spread-of-ebola/. travel restrictions can do more harm than the problems they are meant to resolve for at least three reasons. First, experience with previous health crises reveals that the crises rarely lead to an increase in human mobility. When there is an increase, the movements tends to take place within the country, as people seek to distance themselves from the epicentre of the outbreak. The displacements also tend to be temporary, until people are able to obtain more precise information on the disease. Secondly, the restrictions are inefficient in light of the current dynamics of the transmission of infectious or contagious diseases, which can be spread around the world in only a few days due to the rapid speed of human travel and international trade. This is why the IHR focuses on the adoption of public health measures to control vectors at the points of entry for travel by air, sea or land and the activation of communication channels between states, and not restrictions on the movement of individuals. Finally, travel restrictions and the imposition of measures of isolation upon return hinders the flow of health personnel to regions affected the most, precisely when it is needed the most, thereby affecting the provision of medical supplies and humanitarian aid. On a broader level, the restrictions do considerable damage to the economy of the affected regions, as trade flows are cut off, and to the governments’ capacity to manage the crisis.
It is worth adding that limiting regular entry into destination countries fosters irregular migration. This kind of migration is indeed capable of contributing to the spread of diseases due to the complete absence of control over these people’s presence in a given territory. Furthermore, the climate of rejection towards people from certain places of origin can lead them to not seek treatment for fear that the measures will affect their situation as migrants.
A panel of independent experts suggested that, based on the experience with the Ebola crisis, the WHO should be given the power to sanction states that do not comply with its rules, since undue restrictions cause serious social, economic and political damage to the countries most affected.4242. WHO, “Report of the Ebola Interim Assessment Panel,” July, 2015. In opposition to this suggestion, however, it was argued that the serious flaws in the WHO’s response to the Ebola outbreak incited states to ignore the organisation’s recommendations, as if compliance with the IHR was part of a “political bargain” in which states would only be obliged to comply if the actions of the WHO itself and the most affected countries were flawless in relation to their own obligations.4343. David Fidler, “Ebola Report Misses Mark on International Health Regulations.” Chatham House, July 17, 2015, accessed May 8, 2016, https://www.chathamhouse.org/expert/comment/ebola-report-misses-mark-international-health-regulations. In any case, the fact that countries such as Australia and Canada had adopted restrictions with no consequences reveals that developed countries possess enough political capital to avoid having to fulfil their obligations.4444. Reena Pattani, “Unsanctioned Travel Restrictions Related to Ebola Unravel the Global Social Contract,” Canadian Medical Association Journal 187, no. 3 (Feb 17, 2015):166-167, accessed May 8, 2016, http://www.cmaj.ca/content/187/3/166.full. 4545. In relation to Canada, the eight main destination in the world in terms of the number of international migrants - see: “Migration and Remittances Factbook 2016,” World Bank, 2015, accessed May 8, 2016, http://siteresources.worldbank.org/INTPROSPECTS/Resources/334934-1199807908806/4549025-1450455807487/Factbookpart1.pdf (based on data from 2013 on regular migration). It is worth recalling that due to the Severe Acute Respiratory Syndrome (SARS) outbreak in 2002-2003, the country suffered direct and indirect losses estimated at 2 billion Canadian dollars due to travel restrictions; see: Pattani, “Unsanctioned Travel Restrictions,” 2015.
On the other hand, the possibility of being able to impose sanctions would not resolve the biggest obstacle to complying with the IHR: the incapacity of numerous states – including the countries hit the hardest by the crisis – to fulfil the obligations they assumed under the Regulation due to economic and political constraints.4646. Ventura, “From Ebola to Zika,” 2016. One must recognise that the full implementation of the IHR in West African countries, which would require substantial improvements to the health policies and services that are essential for a life with dignity, would have been much more effective in tackling the causes of a considerable proportion of international migration than restrictions on the circulation of people during the Ebola crisis.4747. Khalid Koser, “International Migration and Global Health Security: Five Lessons From the Ebola Crisis,” The Lancet 385, no. 9980 (2015):1884-1901, accessed Jun. 1, 2016, doi:10.1016/S0140-6736(15)60858-3.
In September 2014, the Secretary General of the United Nations (U.N.) removed the WHO from its role as the coordinator of international action in the field of health by creating the first emergency health mission in history: the United Nations Mission for Ebola Emergency Response (UNMEER).4848. See the main documents related to the UNMEER in “UN Mission for Ebola Emergency Response (UNMEER),” Global Ebola Response, 2014, accessed May 8, 2016, http://ebolaresponse.un.org/un-mission-ebola-emergency-response-unmeer. He did so with the consent of the Security Council and the General Assembly. The Ebola epidemic was from that point considered a threat to world peace and security. Since then, based on the “lessons of Ebola”, the “global health security” approach to international responses to health crisis has been gaining ground has been gaining ground.4949. See, for example, David Heymann et al., “Global Health Security: The Wider Lessons From the West African Ebola Virus Disease Epidemic,” The Lancet 385, no. 9980 (2015): 1884-1901. However, combating the spread of epidemics around the world by strengthening surveillance systems and, when an international response is necessary, deploying U.N. missions focused on contention and militarisation appears to be contributing to the construction of a sort of totalitarian utopia.
It is totalitarian, for one, because it justifies judicial regimes of exception (such as the so-called anti-Ebola laws adopted in the countries affected the most by the epidemic), which undermine democracy and the rule of law. These regimes also sponsor human rights violations that go far beyond the limitations on the exercise of freedoms that could be demanded to prevent diseases from spreading (as is the case of closing real or political borders). It is also totalitarian because when serious health problems are neglected on a global scale – such as malaria, tuberculosis and those affecting the health of women and indigenous peoples, among many others – in order to give priority to the global health security doctrine and combating diseases that are socially constructed as more dangerous, the international response given to the Ebola crisis contributes to greater inequality at the global level.
Secondly, it is utopian. Without going into the vast debate on this concept, the expression is used here to simply refer to an “imaginary representation of a necessary and impossible society”.5050. Jean-Paul Deléage, “Utopies et Dystopies Écologiques,” Ecologie & Politique, no. 37 (2008): 33-43. The strategy of containing diseases by isolating a territory is doomed to failure. Regardless of how large the investments in human and financial resources for surveillance are, the entire physical barrier can potentially be broken. Similarly, the “magic bullet” strategy5151. See, for example, Marcos Cueto, “Chapter One: Malaria and Global Health at the Turn of the 21st Twenty-first Century: A Return to the ‘Magic Bullet’ Approach?,” in When People Come First: Evidence, Actuality, and Theory in Global Health, ed. João Biehl and Adriana Petryna (Princeton: Princeton University Press, 2013): 10-30. – that is, the search for treatment and vaccines that aim to eliminate the disease without tackling the social determinants that, depending on the case, strengthen both the origin and the extent of its propagation – is powerless against the constant mutation of the agents causing the infectious or contagious diseases.
There is a vast literature demonstrating the complexity of the origin of epidemics. Changes in the balance between humans and wildlife, alterations to ecosystems and the increase in exchanges between rural and urban areas, as well as international exchanges, are factors that contribute to the appearance of new diseases. Therefore, the connections between the ecological, epidemiological and socio-economic spheres are fundamental. Disease and epidemics need to be addressed from an integrated ecological view in which humans are treated as one inseparable element of a complex and interactive system.5252. Jean-François Guégan and François Renaud, “Vers Une Écologie de la Santé,” in Biodiversité et Changements Globaux - Enjeux de Société et Défis Pour la Recherche, ed. Catherine Aubertin, Robert Barbault, Bernard Chevassus-au-Louis and Anne Teyssèdre (Paris: ADPF, 2005): 100-116.
For all these reasons, even if restrictions on human mobility could be adopted exceptionally and legitimately by health authorities (and not other authorities), based on scientific proof and while seeking to reduce their negative impact on human rights,5353. This is what Article 32 of the IHR (ibid.) affirms: "In implementing health measures under these Regulations, States Parties shall treat travellers with respect for their dignity, human rights and fundamental freedoms and minimize any discomfort or distress associated with such measures". they are far from being an effective response to the international spread of disease. By way of conclusion, then, one question remains to be answered: what would the response be?
There is no doubt that the risks related to the circulation of people would be radically reduced if states were to give priority to addressing the causes of the persistence and/or the rapid spread of diseases and were capable of both preventing and offering consistent national responses to outbreaks when they are declared.
With regards to resources from international cooperation, the priority should be not only international surveillance systems or programmes to combat specific diseases, but mainly building national health care systems offering universal and free access. This requires investing massive resources for prevention and basic health care in health infrastructure and the recruitment of well-trained, well-paid health professionals with stable careers.5454. The debate on the universal health coverage must be followed carefully. Although it would appear that the WHO’s proposal is to meet this need, it was harshly criticised by various countries, including Brazil, as it appears to serve the interests of the insurance market more than effectively guaranteeing the population’s right to health. See, for example, Paulo Buss et al., “Saúde na Agenda de Desenvolvimento pós-2015 das Nações Unidas,” Cadernos de Saúde Pública 30, no. 12 (2014): 2564-2565, accessed May 8, 2016, http://www.scielo.br/pdf/csp/v30n12/0102-311X-csp-30-12-02555.pdf.
To take global health security seriously – and not just the security of certain developed states – other decisive factors must also be mentioned, such as: urgent and profound changes to the regulation of the production of food and medicines that are capable of subjecting these industries to the need to strengthen public health norms and policies, and a total ban on arms manufacturing and sales which allow existing armed conflicts to continue. These conflicts are largely responsible for the destruction of the rule of law and, consequently, the health systems of the poorest countries, as in the case of Liberia and Sierra Leone. Furthermore, the priority of international action should be the social determinants of health, namely basic sanitation, food, housing and education.
Therefore, the dichotomy that characterises the interface between international migration and health – with the representation of migrants as a threat to health on one hand and the recognition of the vulnerability of the health of migrants who are frequently exposed to difficult working conditions with limited access to rights and policies for inclusion, on the other –5555. Catty Zimmerman et al., “Migration and Health: A Framework for 21st Century Policy-Making,” Plos Medicine 8, no. 5 (2011): e10001034, Jun. 1, 2016, accessed June 3, 2016, http://dx.doi.org/10.1371/journal.pmed.1001034. must be urgently overcome. The international approach to the health of migrants and refugees must be guided by the conflicts at stake in the formulation of national and regional migration policies, but also in the major disputes waged in the global health field,5656. Deisy Ventura, “Mobilidade Humana e Saúde Global,” Revista USP, no.107 (2015): 55-64, accessed May 8, 2016, http://dx.doi.org/10.11606/issn.2316-9036.v0i107p55-64. especially in relation to the inequalities that make it impossible for millions of people today to have a life with dignity in the place where they were born.


